This post got way too long so I have separated out two parts of it into separate short posts to try to make this one more concise. One of them is about what I was wrong with (and a bit right on) with COVID and is here: https://thedebateoverangels.wordpress.com/2023/03/11/covid-vaccines-reasons-to-question-establishment-view/ The other one is about why we should be taking the establishment view on COVID with a grain of salt and can be found here: https://thedebateoverangels.wordpress.com/2023/03/11/covid-vaccines-reasons-to-question-establishment-view/.
Notes to Keep in Mind Before I Begin:
1. I am trying very hard to present both the good and bad with the current vaccines and have tried to double check information for accuracy.
2. Please remember that regardless of your view of the COVID-19 shots in 2021, we are now in 2023 with very different circumstances. We have seen some moves from health departments to recognize the different risk environment. The UK has stopped COVID shots for most under 12. Denmark no longer generally offers boosters for those under 50 (was not a complete stop as some sites took it to be) or a primary series to those under 18. Most of Africa never hit any high vaccination mark and appears to have abandoned trying (its generally younger population was hit very lightly by COVID though).
Later edit: In the weeks since I posted this, Switzerland no longer recommends the COVID shots for anyone and the World Health Organization says healthy kids and teens should not get.
A COVID Vaccine Risk-Benefit Analysis for 2023
Two years ago, we had politicians the world over who wanted a way out of the medical emergency that had been declared. We had a very real disease, incredibly polarized societies as a result of health measures the world over, politicians of every stripe wanting and cheerleading vaccine efforts, pharmaceutical companies who stood to make vast fortunes, agencies who were under extreme pressure to deliver results, and a public demanding a vaccine. In this environment, after real, but very limited research, the health agencies across the world approved the various COVID vaccines and politicians throughout most the world (including basically every major member of both parties here) supported these shots as a way to get back to normal and assured everyone they were “safe and effective.”
Now it’s two years later, and we have a lot more data for both the positive and negative on the COVID vaccines. There are a lot of people who still fully defend the shots and there is also a growing number of experts of a variety of stripes who are raising serious questions. Any possible negative conclusion to those questions would mean egg on the face of pretty much the entire world political class, on every health agency that pushed them, on any businesses or organization that pushed the shots, on anyone in the medical industry who suggested them to patients, on any media which presented the vaccines in an overly positive light, and even on individuals who suggested the shots to friends and family. In that kind of environment, we don’t get good constructive discussions going easily.
Despite this reality, this is a topic I reluctantly write on one final time now and that is for one reason: my conscious. I know people are still getting boosters and still giving shots to children. I am presenting this post because I don’t think most people are getting serious information of the changing risk/benefit analysis with taking a first/boosted COVID shot. I acknowledge that not every accusation against the shots is accurate or backed up and there are positives from the shots (which I will get into), but that being true does not dismiss the evidence we have a problem or mean people should be using the same line of reasoning with the shots today as they did in early 2021.
This post will be broke into 5 parts, Vaccine Background, Vaccine Benefits, What’s Different Now than in 2020, Vaccine Risks, and a Conclusion. I moved what was the original initial part of this post on why we need to be careful taking the establishment view to a different post here: https://thedebateoverangels.wordpress.com/2023/03/11/covid-vaccines-reasons-to-question-establishment-view/ .
I .COVID Vaccine Background
Let’s start with a little background. Viruses vary greatly. Some are highly complex and can’t change in significant ways without them becoming ineffective while others can more easily mutate quickly in larger ways. Some of the highly complex ones can be quite deadly, but they are good candidates to develop vaccines for as the virus is unlikely to change heavily over the years. Most of our quite successful childhood vaccine programs targets these types of viruses.
On the other side, we see viruses which are constantly mutating in larger ways. These are harder to develop effective vaccines for as they can change around protection we try to offer. COVID-19 is caused by the SARS-CoV2 virus which is a coronavirus and, before COVID-19, there was never a successfully created coronavirus vaccine. That doesn’t mean there weren’t attempts. SARS was extremely bad and coronaviruses are bad in animals too. Further, anti-body dependent enhancement (ADE) and original anti-genetic sin (OAS) were problems in a lot of these coronavirus vaccine tries before COVID. With time, in these earlier coronavirus attempts, the viruses shifted and the antibodies response which might have protected from the original strain were now either worthless or actually counterproductive, occasionally in the extreme.
With COVID, the vaccines developed were quite different for these reasons (the way both the andenovector and MRNA shots worked was not even technically as a vaccine until we got a redefinition). Rather than attack the whole virus, they attacked just the spike of the virus hoping to avoid the issues of the past.
The shots were developed quite quickly and initial studies were done over a period of months. Contrary to what was being touted in the media and from politicians, the studies were measuring for one thing and that was reduction in symptoms over this time frame. Each of the eventually emergency approved shots did show positive results while looking at them over that time period and were approved as such.
Like with all things on a societal scale, the vaccines need to be looked with a wider cost-befit analysis. They provided some good and some risk. Let’s now look at both the risk and benefits. We’ll start with benefits.
II. COVID Vaccine Benefits
The Immediate Benefits:
The COVID shots shine brightest shortly after taking them (after 2 weeks anyway). They don’t always stop you getting or transmitting the virus, but even if you do get it, you are less likely to have symptoms and less likely to go to the hospital in the months after the shots. Especially for the oldest part of the population (where risks from COVID were higher and long term risks from the shots mattered less), this is a decent win from the shots all by itself.
How Long?
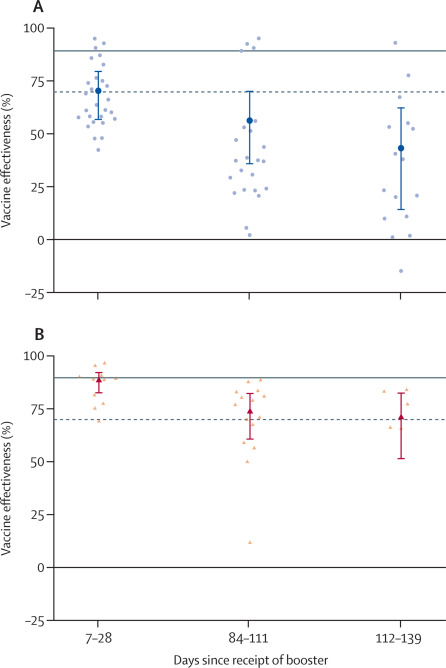
The following graph is out of the Lancet in England. It is putting together a lot of different studies to get a wide feel for the effectiveness of the vaccines. It is also fairly recent, published in February of this year (https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(23)00015-2/fulltext ). The study has serious limitations which I will list below, but it is wide enough in scale to likely fairly accurately show us some of the potential benefits of the COVID shots.

The Bad from the Charts: I used this source because it is such a large amount of studies together that we likely are getting a fairly accurate ranges of data. If I had wanted to cherry pick data (as some on both sides do), I could have easily used one of the outliers. There are two issues that should be noted though:
- Timing: The data is 100 days shy of a year on even the hospitalization data (further on deaths), which doesn’t exactly give us a good long term view.
- While the “all variants” is good to know in a more historical perspective of the pandemic, the omicron sub-variants have pretty much completely replaced all others. So, going forward, we are only really concerned with the omicron data as of now.
The Good from the Charts: Despite those points, the charts do mostly show the shots are lowering risks vs. COVID. The 95% effective claim we got early on about the shots isn’t there, but even against omicron most the later data is showing around a 25% effectiveness against infection which isn’t nothing. Against hospitalization we have stronger data. Even assuming we get some drops with a bit more time, it is probably decently in the positive.
Boosters?
That graph above was just for a primary series. Below is one for after a booster shot. While the boosters do seem to reset protection, they are actually a little less on protection than the primary series after similar time frames. That does suggest less benefit to further shots than the original series, but still benefit.
Newer Shots against Variants
There are of course new shots that are supposed to be better against newer variants. While I would like to see more data, thus far, they seem to temporary help. Against the now dominant sub-variant in the US, “Following bivalent mRNA boosting, responses to XBB.1.5 increase but remain low and wane within 3 months back to pre-boost levels.” https://www.theepochtimes.com/bivalent-covid-vaccines-perform-worse-against-variant-now-dominant-in-united-states-studies_5040659.html?ea_src=ai&ea_med=search
Benefits Conclusion
Whether talking just a primary series, boosters, or new variant booster shots, we can make some conclusions.
- Over the short term, there is definitely utility in the shots for people vs. COVID.
- With time, that utility is still there, but it is shrinking. We don’t know how far it will drop. It has dropped less with hospitalization, but we need longer term data there.
- Taking boosters does appear to provide additional protection for a time period, but that added benefit too declines at a similar or faster rate than an initial series/shot.
- Thus far, we have little reason to believe any new shot will be more effective than any of the previous ones and some reason to believe they will be less effective.
III. Relative Risk in the Population: Now vs. 2020:
In the last section, we talked about potential COVID vaccine benefits. Before we talk about risks, we need to talk about things that have changed now vs. 2 years ago and also about relative risk.
The Different Calculation Now: Omicron and Natural Exposure
There are two key differences in a decision to take or give a COVID shot now vs. when they came out. One is the mutational changes we have seen in the virus and other is that almost all of us have had the actual virus at this point.
Over the years, COVID has mutated, as viruses usually do, to a far less dangerous, but more communicable form. The various omicron sub-variants are basically impossible to stop spreading, but they also are not something that cause the concerns of the original virus or early variants. This doesn’t mean they can’t cause serious complications for some people. They can and do, but, as a whole across society, what we have now is nothing compared to what we started with. An Italian papers estimates a 20 to 40 fold decrease in morality and hospitalization since when we started (https://www.medrxiv.org/content/10.1101/2022.07.01.22277137v1 ). That means that any decisions with taking a COVID shot now must be looked at through that lense and not one of when COVID started.
Further, at this point, the vast majority of people, whether they know it or not, have had COVID. Even by the end of 2020, you can find studies estimating 1/3 of all Americans had had it. In very early 2022 (before omicron had hit initial peaks most places), it was estimated that 57% of the world had been infected at least once (https://www.newsweek.com/covid-evaluation-model-estimates-57-percent-world-population-infected-least-once-1672440 ). Realistically, at this point in time, we are probably talking a single digit percent of the American population who has not had COVID and they are likely ones who do not venture out much. Most people have had it and likely been exposed to COVID multiple times now so it is not something completely new for their body. Further, with increased social activity returning and steadily more transmittable omicron sub-variants, your rate of exposure to the virus is increasing quickly now, not decreasing.
This natural exposure almost everyone has is relevant because it means the body has exposure to the whole virus rather than just the spike and long term memory T cells will provide more protection than you are going to get from exposure to just (an older version) of the spike. The virus is still mutating so this natural exposure is not something that means you can’t get COVID again, but natural infection provides far longer term protection than the various COVID vaccines.
For a visual guide on this look at these graphs out of a different article from the Lancet in England which put together a bunch of studies. The most steady protection by far across the board-past maybe a short period in the beginning-is from natural infection (something almost all of us have had). https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)02465-5/fulltext

Relative Risks
Since the start, we have never fully appreciated the vast gap in how terrible or unalarming a COVID infection could be based on circumstance or why that distinction is important. COVID was literally killing better than 10% of people as it swept through its earliest nursing homes in early 2020. While I generally thought our COVID prevention moves at the time were quite ill advised, I also think we never did enough to protect those in the most vulnerable situations.
As bad as it was for the oldest with the most co-morbilities though, the absolute risk to unvaccinated children was tiny even then and much less now. COVID did kill some and that should not be overlooked or forgotten, but even the BBC reports that in the first 12 months of COVID-19 (when the virus was far worse across society), only 25 under 18 year olds in England died and most of them had very serious issues before that (and many of the rest may well have had undetected issues). (https://www.bbc.com/news/health-57766717 ) You will see some sources trying to suggest a higher mortality rate among children, but this is largely to due to confusing the number of children who died with COVID (a lot of kids who died would also have had COVID given how rampant it was) vs. those dying with COVID as an actual cause (in the US, you would be a COVID death even after an auto crash if you tested positive while at the hospital and the hospital would receive extra federal funding for having a COVID patient).
None of this is to say COVID can’t be bad for the younger groups and that needs to be remembered in treatment, but the relative risk needs to be kept in mind when deciding preventative measures as well. If the risk of serious complications to COVID is incredibly small, then the risk of the vaccines must be even smaller to justify taking. In contrast, there might be more reason for someone in their last year of life to make the decision to take the shot even if it is accepting more risk.
IV COVID Vaccine Risks:
What we were finding out right before the first approved shots made their ways into arms was that there was some worrying research emerging. We got our first, then, non-peer reviewed paper (it was peer reviewed a few months later), saying the spike of the virus was itself pathologic. This was concerning because it was the focal point of the vaccines. Further, while the virus generally had limited ability to transmit the spike to sensitive parts of the body (although in serious cases it could and certain did happen), studies soon showed that the spike from the vaccine was making its way into the blood stream and into places we would rather it not be (the heart and the brain being the most concerning). This was counter to claims at the time that it would not do so.
Some of this would be recognized early. Myocarditis was acknowledged as an issue sometimes in young people. While it was reported most recover, what wasn’t often reported is heart damage is often not something that can just go away. Further, while we were catching the most severe examples out of young adults, there was less reason to think we were catching sub-clinical damage or damage in older age groups.
Let’s look at a few general signs that something is still very off in society health wise and then we will talk a little more specifically about heart concerns.
General Red Flags
1. VAERS: The Vaccine Adverse Events Reporting System (VAERS) was created by Congress in the 1980s after vaccine manufacturers were given liability protection. The system has a lot flaws, but also its uses. Being reported on it does not mean an injury has to be vaccine related; it might just be coincidence in timing. On the flip side, it takes work and effort to get something reported (as well as attributing the issue to a vaccine in the first place), so it is estimated a very, very large majority of issues never make the list. From 2007-2010, the Harvard Pilgrim Health Center did a study that estimated less than 1% of vaccine adverse events were reported to VAERS (https://rickjaffeesq.com/wp-content/uploads/2021/02/r18hs017045-lazarus-final-report-20116.pdf ). Deaths were probably reported far more accurately and I suspect we have upped the average for other issues over the years, but we probably still have a big under-report.
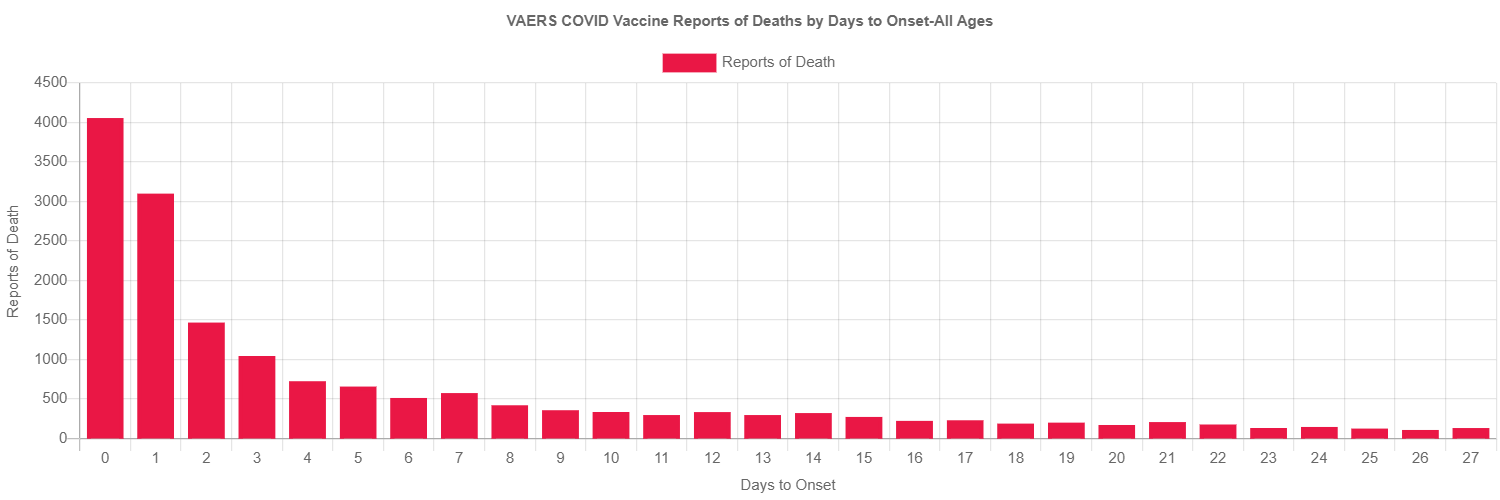
Still, there is useful information from VAERS. While COVID vaccine injuries should be large as the shots have been used in a large number of people, it is not like the flu shot numbers or childhood vaccine numbers are small and, over the years, we have a lot of vaccines that get reported for occasional major side effects. Even though the evidence for most approved vaccines is that the benefits far outweigh the risks, there are always some people who react very badly for one reason or another (no medical procedure is without risks). All this said, look at the chart below on deaths reported to VAERS. The deaths reported to the system from COVID vaccines has to be taken as at least a serious red flag. While the evidence might not be conclusive enough to make definitive conclusions about the safety of the COVID shots, it would warrant enough concern to likely get most other vaccines pulled.

Source for both graphs: https://openvaers.com/covid-data
Here is a breakdown by numbers and how many days after a COVID shot.
Beyond deaths, we see similar type rise in reports of other adverse events. Data out of Florida showed 4x more vaccines taken with the COVID shots over a period, but a 1700% increase in adverse event reporting. It also reported a 44x increase in life threatening conditions after a taking a shot (https://www.youtube.com/watch?v=V2YGdDbZpSg ).
Again there is caution on some of this data as an increase use of VAERS (which is supposed to be mandatory since the 80s, but practically is underutilized) could explain some of it and we have never really known how accurate it was with deaths. That said, it is difficult to look at the data without at least coming to the conclusion that the COVID shots carry more risk than any other vaccines currently available in this country.
2. Excess Death
Trying to measure exactly what kills people is more complex than it sounds like it should be. Sometimes it is multiple things, sometimes it is something different than we think, and sometimes we really just don’t know. One way we can try to measure public health measures though is by looking at excess deaths across the whole of society.
Excess Deaths are, as the name implies, deaths above the number we expected for a given time. This can sound cold, but based on large populations, you can figure roughly how many people would normally die over periods of time given demographics and statistics and usually the number is pretty spot on. It can be above or below for awhile based on various things though. If you get a really bad flu year for example, it will kill people who wouldn’t have died otherwise and we will have excess deaths. On the other side of that coin, if we have multiple years of lighter flu outbreaks, we have fewer vulnerable deaths and have a negative excess death number.
Over time, the excess death number should balance out to about zero. Maybe we had a really bad flu year and it gave us a lot of excess deaths. After that though, there will be fewer vulnerable people the following year and we will have smaller than average deaths accordingly. If we get lucky and have many years of light flu seasons and see fewer excess deaths, then we have increased the number of vulnerable people and will have a higher excess death rate when we finally do have a worse flu outbreak.
Here is a chart using CDC data:

Source: https://www.usmortality.com/deaths/excess-yearly-cumulative
Look at the various years there. From 2015 to March of 2020, we stuck right along the baseline and no year was off by more than 20,000 either direction. Unsurprisingly, we started to see an uptick in excess deaths in March of 2020 due to COVID directly and to our response to COVID (delayed treatments, not going to doctors/hospitals, and increased risky behavior contributed to the higher death toll in addition to direct COVID deaths). For most the rest of 2020, the excess death could be put squarely on those two factors. By late 2020, we were putting the first shots in arms and this would be going on in earnest in early 2021. By late spring, pretty much anyone in American who wanted a shot had one. We also had delta as the dominant strain which was worse than previous strains.
While the excess deaths those first two years could be explained by just COVID, the high excess death rate in 2022 is harder to justify. We already had high excess death for two years and, by the law of averages, should have been dropping well below zero to balance that out (at least as far as deaths were among the vulnerable) outside of a good explanation. At this point, the omicron variant was dominant and it was far more mild than any of the other variants had been. Further, the vast majority of the population had now had at least two shots.
This to me is another red flag that something is off. Again it is not a proof positive the vaccines are to blame as you could offer other explanations, but when you add it with things like life insurance companies coming out saying there was 40% increase in non-COVID deaths for working age adults during part of this time period, it is definitely a red flag that is not easily explained.
If you want to see some other world wide numbers, Dr. John Campbell, goes through a bunch of them here. https://www.youtube.com/watch?v=av4Ej6om0WI Side note: This doctor had two COVID shots and a booster and, for a long time, had a sign up in every video about the importance of masks, hand washing, and the like (until Omicron started and changed the calculation). I started following him as, even though I didn’t agree with everything he was saying, I greatly respected how his channel was taking peer reviewed research and was diving into it. The more he reviewed, the more you can tell his tone has changed on the vaccines even though he will strictly follow Youtube guidelines (which do limit your ability to talk about issues with the vaccines).
Longer Term Issues Showing Up
There are a lot of arguments about what the various COVID shots effect in negative ways and other long term potential issues. Rather than focus on the validity all of them (I have not researched enough to comment on most of them), I am going to focus just on the one that I think is the most concerning and I think has the most compelling arguments. That is the unintended bad effects of the various COVID shots related to the heart.
There are reasons we should be concerned about the various COVID vaccines effecting the heart in ways that COVID itself was less likely to. Despite initial claims, we know the spike protein (which was found to be pathologic itself right before we started mass vaccination) created from the MRNA jabs does go into the blood stream. A study found it was in the blood stream in 11 out of the 13 participants after a Moderna shot (https://academic.oup.com/cid/article/74/4/715/6279075 ). This goes counter to claims at the time that it would not enter the blood stream. From there, there is room for it to effect areas of the body well beyond around the injection site. This generally gives the shots far further reach into the body than natural infection does (where only severe cases see it spread as far). We even have recent additional evidence on this front as a study out of Denmark showed that mRNA generated spike still in the blood after 28 days, way longer that expected ( https://onlinelibrary.wiley.com/doi/10.1111/apm.13294 ).
Further, while articles have shown up tying COVID infections (rather than the vaccines) to heart issues of late, the evidence isn’t there for COVID being special in creating them (https://www.statnews.com/2021/05/14/setting-the-record-straight-there-is-no-covid-heart/ ). “Numerous research groups published studies that refuted the early concerns and provided reassuring evidence that SARS-CoV-2 had no extra toxicity to the heart.“ A COVID infection can cause heart issues, but it is not really special in anyway amongst respiratory viruses in being able to.
Direct Evidence: A Study from Thailand, Switzerland, and other American data
There has been limited published studies that look for heart damage from the vaccines. This is probably because there are very few who will benefit if they come back negative. That said, there was one big one done in Thailand. https://www.preprints.org/manuscript/202208.0151/v1 The study looked at over 300 teens and found cardiovascular effects in just under 30% of those who took the vaccine. While most do not have immediate significant risk, the stat is still alarming. Seven of the participants (2.33% of all including those they lost contact with) had myocarditis or pericarditis with 3 (just under 1%) enough to be symptomatic. Those numbers may not sound large, but given the small risk COVID is to the age group, they are not something that can simply be ignored. The numbers look worse if looking at just males.
From Switzerland, we have another study that suggests 3% of vaccinated or boosted young people develop, “mild damage to the heart muscle cells.” https://www.theepochtimes.com/mit-expert-calls-for-immediate-stop-of-mrna-covid-jab-evidence-shows-unprecedented-level-of-harm_5020151.html?ea_src=ai&ea_med=search
Looking further into American data, we see that heart and vein issues among 25 to 44 year olds in 2022 is still 13% over the 2019 baseline while other age groups have receded back to norms (https://www.theepochtimes.com/heart-vein-disease-deaths-high-in-25-44-year-olds_5010722.html?ea_src=ai&ea_med=search ). According to Josh Stirling, an insurance research analysis, when talking about mortality in general, he said, “The more doses on average you have in a region within the United States, the bigger increase in mortality that region has had in 2022 when compared to 2021.”
Indirect Evidence: Athletes and Pilots
Let’s look at a couple simple indirect examples that shows something has changed to add heart risks in society. We’ll start with soccer. Soccer is the biggest sport in the world and a team sport with almost constant cardio activity as teams run across the field all game with limited breaks. Dr. Josh Guetzkow, a senior lecturer in the Department of Sociology and Anthropology at the Hebrew University’s Institute of Criminology in Israel has researched the rate of Sudden Cardiac Death (SCD) and Sudden Unexplained Death (SUD) collapses on FIFA soccer fields. He has determined that deaths on the field across the world have increased by a factor of 5. (https://diariodevallarta.com/en/sudden-and-unexplained-cardiac-deaths-among-fifa-players-in-2021/ ). You would expect about 5 deaths across the world per year due to sudden heart issues given the number of players (only moderately changed since 2000) and the rarity of the event. From 2001 to 2020 that was close to correct with about 4.2 per year. In 2021 though, there were 21 cases. This is not the extreme some are making it out to be, but a 5 fold increase over the baseline is not something to take lightly and further changes should be looked at very closely rather than be dismissed.
Airline pilots have some of the strictest health standards for their job out there. The FAA and other organizations across the planet, really, really do not like anything that can incapacitate a pilot. As such, pilots have to pass fairly strict heart monitoring processes. There had been rumors I had read after the COVID shots of pilots no longer able to fly. That is not something I would post in this blog though (not enough verification or context), except for now the FAA has very quietly and without explanation increased their EKG limit by 50% (https://www.ntd.com/faa-change-to-heart-test-limit-triggers-worries-over-pilot-health-public-safety_896864.html). They have not offered explanation, but it is obvious pilot shortages are a real concern. Maybe this is simply the easiest fix they can find to the issue, but the timing can’t be ignored completely either. The fact they won’t comment on this doesn’t make me feel more comfortable either.
Conclusion:
This is all just my reading of the tea leaves over the last few years. The COVID vaccines have provided some help to people, but I think the amount of help they have provided is being overstated, the risks understated, and the changes with time not being well communicated. If you are considering further COVID shots or getting them a 1st time, please consider the arguments here and others from sources that are critical of the shots as well as from media which is still almost entirely positive on them. If you conclude the benefits outweigh the risks to a shot/an additional shot then take them, but do so because that is your conclusion based on the evidence.
With that, I believe I can finally let COVID go. Thanks to anyone who read this far. Two attached posts at the top for anyone interested.
